
The Silent Epidemic: Why Chronic Inflammation Matters
Inflammation is a double-edged sword. Acute inflammation — the redness, swelling, and heat after an injury — is your immune system working exactly as designed. But when inflammation becomes chronic — a low-grade, systemic, smoldering fire that never extinguishes — it becomes the common thread connecting the world's most devastating diseases.
Chronic inflammation is now recognized as a central driver of:
| Condition | Global Burden | Inflammatory Mechanism |
|---|---|---|
| Osteoarthritis | 528 million people | Cartilage degradation via IL-1β and TNF-α |
| Rheumatoid Arthritis | 18 million | Autoimmune synovial inflammation |
| Cardiovascular Disease | Leading cause of death globally | Endothelial NF-κB activation |
| Type 2 Diabetes | 537 million adults | Adipose tissue inflammation, insulin resistance |
| Chronic Pain | 20% of adults worldwide | Neuronal inflammation and central sensitization |
| Neurodegeneration | 50 million with dementia | Microglial NF-κB activation |
The anti-inflammatory therapeutics market — valued at $109.58 billion in 2024 — reflects the scale of this problem. Yet NSAIDs, the most prescribed class, come with well-documented risks: gastrointestinal bleeding, cardiovascular events, and renal toxicity with long-term use. This is where quercetin enters the picture — not as a replacement, but as a fundamentally different approach to inflammation.
NF-κB: The Master Switch of Inflammation
To understand how quercetin works, you must first understand NF-κB.
NF-κB (Nuclear Factor kappa-light-chain-enhancer of activated B cells) is a protein complex that acts as the central command center for inflammatory gene expression. When a cell detects danger — a pathogen, tissue damage, oxidative stress, or inflammatory cytokines — NF-κB translocates from the cytoplasm into the nucleus, where it binds to DNA and switches on the production of pro-inflammatory genes.
The NF-κB activation cascade follows a well-defined sequence:
Inflammatory Trigger (LPS, TNF-α, IL-1β, oxidative stress)
↓
IκB kinase (IKK) activation
↓
IκBα phosphorylation and degradation
↓
NF-κB (p50/p65) release
↓
Nuclear translocation of NF-κB
↓
Gene transcription of inflammatory mediators
┌──────────┬──────────┬──────────┬──────────┐
│ TNF-α │ IL-6 │ IL-1β │ COX-2 │
│ iNOS │ MCP-1 │ MMP-9 │ NLRP3 │
└──────────┴──────────┴──────────┴──────────┘
In healthy tissue, this pathway is tightly regulated. In chronic inflammatory disease, it runs unchecked — NF-κB stays constitutively active, continuously pumping out inflammatory cytokines that recruit more immune cells, which produce more NF-κB-activating signals. It's a self-perpetuating loop.
How Quercetin Blocks NF-κB: A Multi-Target Interception
Quercetin does not block NF-κB at a single point — it intercepts the inflammatory cascade at multiple levels simultaneously, which explains its potency as an anti-inflammatory compound.
Mechanism 1: AKT1-FoxO1 Pathway — The Primary Target
A landmark 2024 study published in Nature Scientific Reports used molecular docking, network pharmacology, and in vivo validation to map quercetin's anti-inflammatory mechanism. The findings were striking:
Molecular Docking Results:
| Target Protein | Total Score | Role in Inflammation |
|---|---|---|
| AKT1 | 8.35 (highest) | Master kinase, activates NF-κB via IKK |
| KDR | >7.0 | VEGF receptor, vascular inflammation |
| EGFR | >7.0 | Growth factor signaling, tissue remodeling |
| CDK1 | >7.0 | Cell cycle, inflammatory proliferation |
| PIK3R1 | >7.0 | PI3K regulatory subunit, upstream of AKT |
| SRC | >7.0 | Tyrosine kinase, inflammatory signaling |
| MMP9 | >7.0 | Matrix degradation in arthritis |
Quercetin's highest affinity was for AKT1 (Total Score: 8.35). When quercetin binds AKT1, it promotes AKT1 phosphorylation, which in turn phosphorylates FoxO1 — tagging it for nuclear exclusion. Here's why that matters:
- FoxO1 in the nucleus → promotes TLR4/MyD88/MD2 expression → activates NF-κB → triggers inflammation
- FoxO1 phosphorylated by AKT → exits the nucleus → TLR4/MyD88/MD2 pathway silenced → NF-κB stays inactive
In macrophage experiments (Raw264.7 cells stimulated with LPS), quercetin at 2.5–10 μg/mL produced concentration-dependent suppression of:
- TLR2 and TLR4 receptor expression
- MyD88 adaptor protein levels
- Nuclear FoxO1 accumulation (confirmed by immunofluorescence)
- Downstream NF-κB-dependent gene transcription
Mechanism 2: Direct JAK/STAT Pathway Inhibition
A 2025 study in Molecular Biology Reports revealed a second axis: quercetin directly inhibits the JAK/STAT signaling pathway, which runs parallel to NF-κB and amplifies inflammatory cytokine responses.
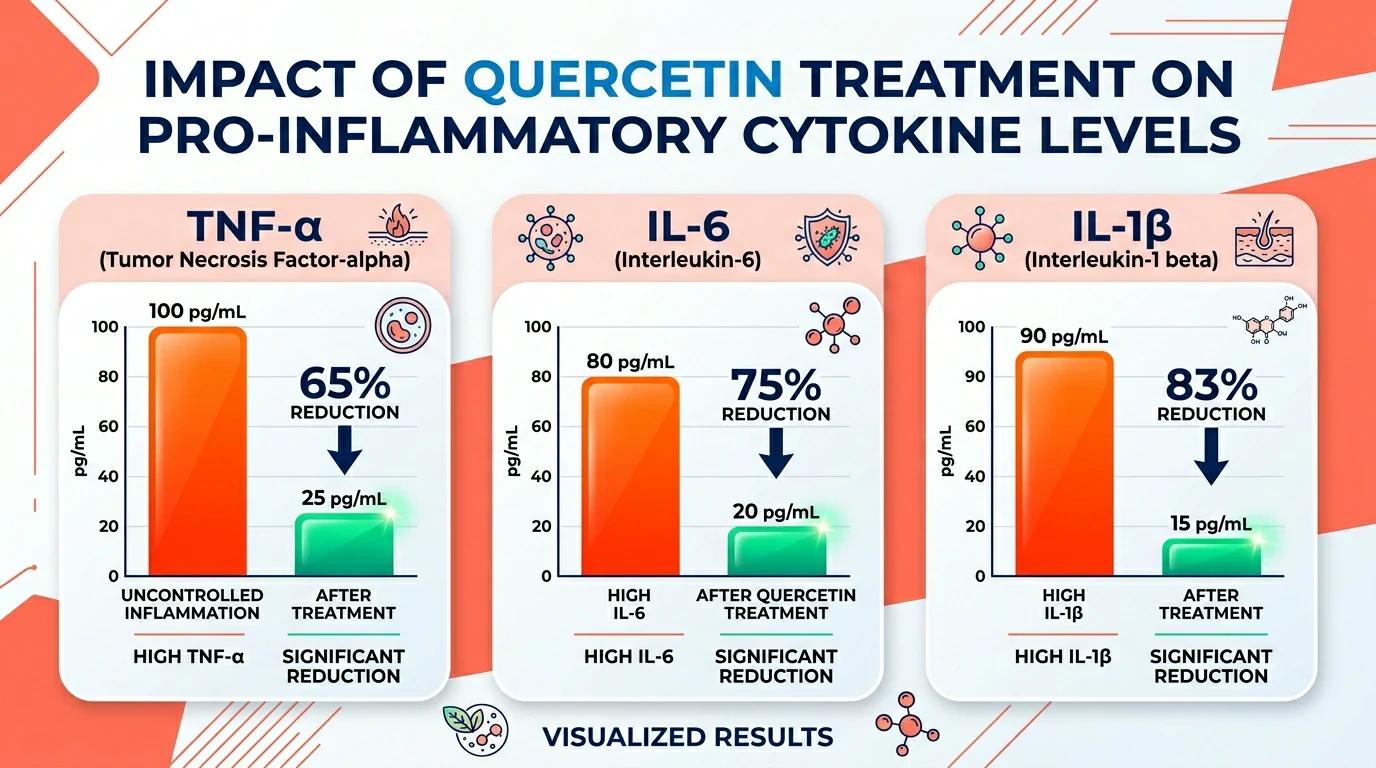
In LPS-stimulated macrophages, quercetin treatment resulted in:
| Inflammatory Mediator | Effect of Quercetin | Clinical Significance |
|---|---|---|
| TNF-α | Dose-dependent suppression | Primary driver of rheumatoid arthritis synovitis |
| IL-6 | Dose-dependent suppression | Key mediator of CRP production, chronic inflammation marker |
| IL-1β | Dose-dependent suppression | Central to osteoarthritis cartilage degradation |
| IL-8 | Dose-dependent suppression | Neutrophil chemoattractant, tissue damage |
| COX-2 | Suppressed at gene level | Reduces prostaglandin E2 synthesis |
| iNOS / NO | 24h & 48h dose-dependent reduction | Reduces nitric oxide-mediated tissue damage |
| MCP-1 | Dose-dependent suppression | Monocyte recruitment, atherosclerotic plaque formation |
Critically, quercetin reduced intracellular ROS levels — from approximately 70% (LPS alone, 24h) and 90% (LPS alone, 48h) — in a concentration-dependent manner, demonstrating that its anti-inflammatory mechanism is coupled with direct antioxidant activity.
Mechanism 3: NLRP3 Inflammasome Suppression
The NLRP3 inflammasome is a multi-protein complex that acts as the cellular "panic button" — when activated, it triggers caspase-1 cleavage and the release of mature IL-1β and IL-18, driving pyroptosis (inflammatory cell death). NLRP3 is implicated in gout, atherosclerosis, Alzheimer's disease, and type 2 diabetes.
The 2025 Springer study confirmed that quercetin prevents NLRP3 inflammasome activation in macrophages, adding a third layer to its anti-inflammatory mechanism. By blocking NLRP3 assembly, quercetin prevents the amplification loop where IL-1β release further activates NF-κB in neighboring cells.
The Three-Layer Anti-Inflammatory Model
These mechanisms operate as a coordinated, multi-level defense:
QUERCETIN
│
┌───────────────┼───────────────┐
│ │ │
LAYER 1 LAYER 2 LAYER 3
AKT1-FoxO1 JAK/STAT + NLRP3
Pathway NF-κB Direct Inflammasome
│ │ │
FoxO1 nuclear Cytokine gene IL-1β maturation
exclusion → suppression → blocked →
TLR4/MyD88 TNF-α ↓ No pyroptosis
silenced IL-6 ↓ No amplification
IL-1β ↓
│ │ │
└───────────────┼───────────────┘
↓
Inflammation Suppressed
This multi-target approach is pharmacologically significant: unlike single-pathway drugs that cells can bypass through redundant signaling, quercetin's broad interception makes it difficult for inflammatory cascades to route around.
Macrophage Polarization: Shifting from M1 to M2
Beyond blocking inflammatory signaling, quercetin actively reprograms immune cell behavior. Macrophages exist on a spectrum:
- M1 (pro-inflammatory): CD40+ CD80+ phenotype, produces TNF-α, IL-6, ROS — drives tissue damage
- M2 (anti-inflammatory): CD163+ CD206+ phenotype, produces IL-10, TGF-β — drives tissue repair
In the 2024 Nature Scientific Reports study, LPS stimulation pushed approximately 70% of macrophages into the CD40+ CD80+ M1 phenotype. Quercetin treatment (10 μg/mL) significantly reduced this proportion, as confirmed by both surface marker analysis (flow cytometry) and CD40/CD80 mRNA quantification. This M1→M2 shift means quercetin not only silences inflammation — it actively promotes tissue healing.
Chronic Pain and Arthritis: Clinical Relevance
Arthritis
A 2024 scoping review in Beyond Rheumatology systematically evaluated quercetin across four rheumatological conditions:
| Condition | Key Finding |
|---|---|
| Rheumatoid Arthritis | Quercetin inhibited synovial fibroblast proliferation and reduced MMP expression, protecting joint architecture |
| Osteoarthritis | Suppressed IL-1β-induced chondrocyte apoptosis and matrix metalloproteinase (MMP-13) production |
| Gout | Reduced uric acid levels and NLRP3-mediated joint inflammation |
| Pre-hyperuricemia | Inhibited xanthine oxidase, reducing uric acid production |
In preclinical models, quercetin reduced paw swelling, joint destruction scores, and serum inflammatory markers. The mechanism consistently traced back to NF-κB suppression in synovial tissues.
Chronic Pain
A 2025 comprehensive review in ScienceDirect highlighted quercetin's analgesic potential: by repressing neuronal inflammation and oxidative stress, quercetin addresses the neuroinflammatory component of chronic pain — the mechanism behind central sensitization, where pain persists long after the initial tissue injury has healed.
This is particularly relevant for conditions like fibromyalgia, neuropathic pain, and chronic lower back pain, where traditional anti-inflammatories often provide limited relief.
Quercetin vs. NSAIDs: Upstream vs. Downstream
| Feature | NSAIDs (Ibuprofen, Naproxen) | Quercetin |
|---|---|---|
| Target | COX-1/COX-2 enzymes (downstream) | NF-κB transcription (upstream) |
| Mechanism | Blocks prostaglandin synthesis | Suppresses COX-2 gene expression |
| Effect on IL-6/TNF-α | Minimal direct effect | Direct suppression |
| Effect on NLRP3 | Minimal | Direct inhibition |
| GI side effects | Significant (COX-1 inhibition) | None reported |
| Cardiovascular risk | Present with long-term use | No evidence of risk |
| Tissue repair | May impair healing | Promotes M2 macrophage polarization |
| Duration of safe use | Limited (weeks-months) | Suitable for long-term use |
The complementary nature is clear: NSAIDs work fast by blocking the final enzyme, while quercetin works at the transcriptional root. For chronic inflammatory conditions, this upstream mechanism is arguably more sustainable.
Anti-Inflammatory Cytokine Profile: What Gets Suppressed and Why
| Cytokine | Function in Inflammation | Disease Relevance | Quercetin Effect |
|---|---|---|---|
| TNF-α | Master pro-inflammatory cytokine | RA, Crohn's, psoriasis, atherosclerosis | Gene-level suppression |
| IL-6 | CRP induction, Th17 differentiation | Cardiovascular disease, COVID-19 cytokine storm | Dose-dependent reduction |
| IL-1β | NLRP3-dependent release, pyrexia | Gout, OA, type 2 diabetes | Blocked at NLRP3 + gene level |
| COX-2 | Prostaglandin E2 synthesis | Pain, fever, cancer | Transcriptional suppression |
| iNOS | NO production, tissue damage | Septic shock, neurodegeneration | mRNA and protein reduction |
| MCP-1 | Monocyte recruitment | Atherosclerosis, obesity | Dose-dependent suppression |
| MMP-9 | Extracellular matrix degradation | Arthritis, cancer metastasis | Gene-level suppression |
How to Use Quercetin for Inflammation: Evidence-Based Dosing
| Health Goal | Daily Dose | Co-Factors | Duration for Results |
|---|---|---|---|
| General anti-inflammatory maintenance | 500 mg | Bromelain 100 mg | 4–8 weeks |
| Arthritis / joint pain | 500–1,000 mg | Bromelain 100–200 mg, Vitamin C 500 mg | 8–12 weeks |
| Chronic pain / neuroinflammation | 800–1,000 mg | Bromelain 150 mg, Curcumin optional | 8–12 weeks |
| Gout / hyperuricemia | 500–1,000 mg | Vitamin C 500 mg | 4–8 weeks |
| Post-exercise inflammation | 500 mg | Taken 60 min before exercise | Acute (hours) |
Form selection matters: Standard quercetin dihydrate has low oral bioavailability (~2%). Quercetin phytosome (Indena's Quercefit) and EMIQ (enzymatically modified isoquercitrin) offer 10–20× higher absorption. For anti-inflammatory applications, these enhanced forms reduce the required dose and accelerate onset of effects.
Request a sample or product specification →
Safety and Drug Interactions
Quercetin is generally well-tolerated at 500–1,000 mg daily. Documented considerations:
- Blood thinners (warfarin): Quercetin may affect CYP2C9, potentially altering warfarin metabolism — monitor INR
- Chemotherapy agents: Quercetin's antioxidant activity may theoretically interfere with pro-oxidant chemotherapy mechanisms — consult oncologist
- Corticosteroids: Potential additive anti-inflammatory effect — monitor for excessive immune suppression
- Cyclosporine / tacrolimus: May affect metabolism via CYP3A4 — monitor drug levels
No significant adverse effects were reported in the 1,002-person quercetin URTI trial at 1,000 mg/day for 12 weeks.
Last updated: May 2026. This article is for informational purposes and does not constitute medical advice. Always consult a healthcare professional before starting any supplement regimen.
Source: This article references peer-reviewed research published in Nature Scientific Reports (2024), Molecular Biology Reports (2025), Inflammopharmacology (2025), ScienceDirect (2025), and the Beyond Rheumatology scoping review (2024).
Related Articles
- Free Radicals vs. Quercetin: The Antioxidant Mechanism Explained — The antioxidant-to-anti-inflammatory cascade
- Quercetin for Gut Inflammation: From Leaky Gut to IBD Support — Gut-specific inflammatory pathways
- Quercetin Safety Profile: Dosage, Drug Interactions, and Who Should Avoid It — Long-term safety for chronic inflammation management
Explore high-purity quercetin extract from Sophora japonica at ginkvora.com/products/quercetin — standardized to ≥95% quercetin for consistent anti-inflammatory formulation.