
TL;DR
PDRN, exosomes, EGF, retinol, and peptides are often discussed as competing "regenerative" skincare technologies — but they work through fundamentally different mechanisms and carry vastly different levels of clinical evidence. This article compares them head-to-head: mechanism, published data, safety profile, cost, and regulatory maturity. The short version: PDRN has the strongest clinical evidence in the regenerative category (20+ years, multiple RCTs), making it the most defensible choice for evidence-based brands. Exosomes have more theoretical potential but no large-scale human trials. Retinol remains the gold standard for cell turnover but causes irritation that PDRN avoids. Peptides are the surgical tool — precise, targeted, but narrow. EGF has efficacy data but regulatory hurdles. Each has a role, and the smartest formulations often combine them.
PDRN vs Exosomes: The Main Event
This is the comparison generating the most interest in aesthetic dermatology — and for good reason. Both are marketed as "regenerative" technologies that go beyond surface-level skincare to stimulate tissue repair at the cellular level. But the science behind them, and the evidence supporting them, could not be more different [1][2].
Mechanism
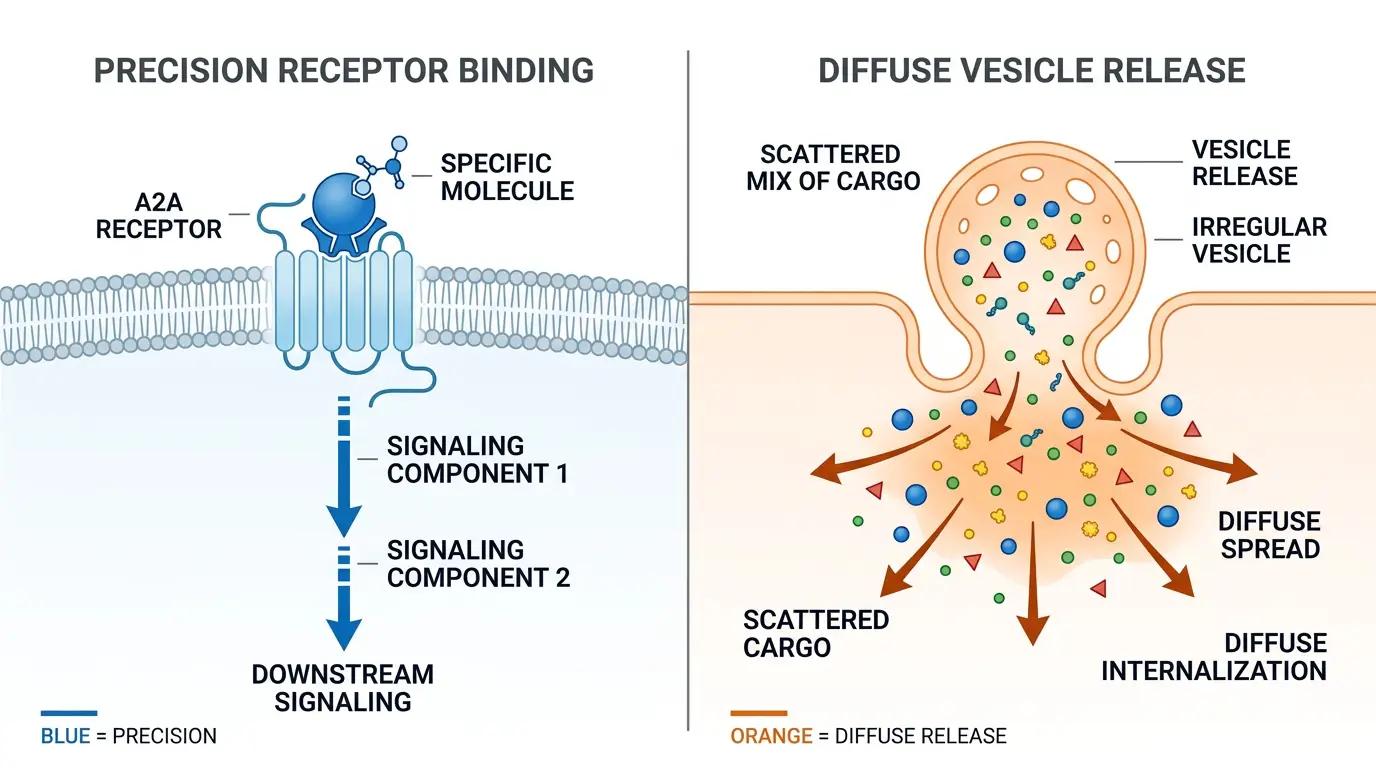
PDRN activates a specific receptor — the adenosine A2A receptor (A2AR) — through its degradation product adenosine. This triggers a well-characterized signaling cascade: A2AR → adenylyl cyclase → cAMP → PKA/Epac2 → downstream effects including NF-κB suppression (anti-inflammatory), VEGF upregulation (pro-angiogenic), and fibroblast activation (pro-collagen). It is a single-molecule, single-receptor mechanism with predictable pharmacology [1].
Exosomes deliver a complex and variable molecular cargo — proteins, lipids, mRNAs, microRNAs — from their parent cells (usually mesenchymal stem cells) to recipient cells. The exact effect depends on what is in the cargo, which depends on the source cell type, culture conditions, isolation method, and storage conditions. There is no single "exosome mechanism" — each exosome preparation is functionally a different product [2].
Clinical Evidence
This is where the gap is widest.
PDRN has:
- Double-blind RCTs: 216 patients (diabetic ulcers), 218 patients (facial rejuvenation), plus multiple smaller trials
- Systematic reviews: Multiple published meta-analyses
- Clinical use: 20+ years with consistent, reproducible results across different populations and protocols
- Specific outcomes: 61.4% wrinkle reduction at 12 weeks, 37.3% vs 18.9% complete wound healing (p = 0.0027) [1]
Exosomes have:
- Preclinical studies: In vitro and animal model data — promising but not yet translated to human RCTs
- Case series: Small, typically uncontrolled, often industry-funded
- Zero large-scale double-blind RCTs published for aesthetic indications
- The International Society for Extracellular Vesicles (ISEV) has published MISEV guidelines specifically because exosome research suffers from reproducibility and standardization problems [2]
Standardization
PDRN is a chemically defined product. Every batch of salmon-derived PDRN contains DNA fragments in the 50–2,000 bp range with >95% purity and an OD 260/280 ratio of 1.8–2.0. Different manufacturers' products (Rejuran, Nucleofill, Plinest, Placentex) use chemically similar material and produce clinically similar results [1].
Exosomes have no standardized active molecule. The cargo of an exosome varies with every variable in the production process — source cell type, passage number, culture media, harvesting method, storage conditions. Two "exosome serums" on the market may have completely different biological effects because their cargoes are different [2].
Cost and Accessibility
- PDRN injectable: $200–500 per session
- PDRN topical: $15–60 per product
- Exosome injectable: $500–2,000+ per session
- Exosome topical: $50–200+ per product
Verdict
For evidence-based brands: PDRN. For speculative, future-oriented brands with risk tolerance: exosomes — with the understanding that the clinical data is not there yet. The most sophisticated approach may be combining them: PDRN as the evidence-backed regenerative foundation, exosomes as an adjunctive growth factor booster. Korean dermatologists are already exploring this combination, with the theoretical rationale that the two mechanisms are complementary (A2AR activation + growth factor delivery), though dedicated combination trials have not yet been published.
PDRN vs EGF: Proliferation vs Regeneration
Epidermal Growth Factor (EGF) is a 53-amino acid polypeptide that directly stimulates cell division by binding to the EGF receptor (EGFR) on the surface of keratinocytes and fibroblasts. It was discovered in 1986 (earning a Nobel Prize) and has been used topically in cosmetic and medical contexts — particularly in Asia — for wound healing and anti-aging [3].
Mechanism Comparison
| Dimension | PDRN | EGF |
|---|---|---|
| Target Receptor | Adenosine A2A receptor (GPCR) | EGF receptor (tyrosine kinase) |
| Primary Effect | Multi-pathway regeneration (anti-inflammatory + angiogenic + collagen) | Cell proliferation (mitogenic) |
| Signaling Breadth | Broad (NF-κB, VEGF, TGF-β, cAMP/PKA) | Narrow (Ras/MAPK, PI3K/AKT) |
| Anti-inflammatory | Yes (NF-κB suppression) | Minimal |
| Angiogenesis | Yes (VEGF upregulation) | Indirect |
EGF's mechanism is simpler and narrower: it tells cells to divide. This is valuable for wound healing but less comprehensive than PDRN's multi-pathway approach, which simultaneously reduces inflammation, builds new blood vessels, and stimulates collagen production — repairing tissue architecture rather than just increasing cell count.
Regulatory Status
PDRN has clearer regulatory pathways: approved as a pharmaceutical/medical device in multiple markets (Korea MFDS, EU CE-mark). EGF occupies a more ambiguous space — it is a potent growth factor, and some regulators treat topical EGF products with caution due to theoretical concerns about uncontrolled cell proliferation, particularly in individuals with undiagnosed skin cancers. While no causal link between cosmetic EGF and cancer has been established, the regulatory uncertainty has limited EGF's market penetration compared to PDRN, particularly in Western markets.
Verdict
PDRN offers a more comprehensive regenerative effect with better regulatory positioning. EGF excels in wound healing contexts but carries regulatory baggage that PDRN avoids. For formulators choosing between them, PDRN is generally the lower-risk, better-evidenced option for cosmetic applications.
PDRN vs Retinol: Regeneration vs Renewal
Retinol (vitamin A) is the most extensively studied anti-aging ingredient in dermatology, with decades of clinical data supporting its effects on fine lines, hyperpigmentation, and skin texture. Its mechanism — binding to nuclear retinoic acid receptors (RAR/RXR) to regulate gene transcription — is fundamentally different from PDRN's cell-surface A2A receptor pathway [4].

Mechanism
Retinol accelerates epidermal turnover by upregulating genes involved in keratinocyte differentiation and desquamation. It also stimulates collagen synthesis in the dermis, though this effect is mediated through the same nuclear receptor pathway rather than a dedicated regenerative receptor. The visible improvement in skin texture comes primarily from accelerated shedding of the stratum corneum — it literally thins and renews the outer layer of skin [4].
PDRN does not accelerate cell turnover. It stimulates tissue repair through receptor-mediated signaling, improving the quality of the extracellular matrix rather than the speed of epidermal renewal. There is no "retinization" period, no peeling, and no photosensitivity.
The Irritation Gap
This is the most practical difference for product formulators:
| Characteristic | PDRN | Retinol |
|---|---|---|
| Adjustment Period | None | 2–4 weeks ("retinization") |
| Irritation | None | Common (dryness, peeling, redness) |
| Photosensitivity | None | Yes (requires SPF) |
| Pregnancy Safe | Yes (non-systemic) | Contraindicated |
| Sensitive Skin | Well-tolerated | Often poorly tolerated |
| Results Onset | Gradual (4–12 weeks) | Textural (4–6 weeks), anti-aging (12+ weeks) |
For consumers who cannot tolerate retinol — an estimated 30–50% of people who try it — PDRN offers a regenerative alternative without the trade-off of irritation. For consumers who can tolerate retinol, the two can be used on alternate nights for complementary benefits.
Combining PDRN and Retinol
The two ingredients are mechanically compatible and complementary:
- Retinol: Accelerates cell turnover, revealing fresher skin
- PDRN: Stimulates tissue repair, improving the quality of the newly revealed skin
A common protocol is retinol on night 1, PDRN on night 2, rest/recovery on night 3. This avoids over-exfoliation while maintaining consistent regenerative signaling.
Verdict
Retinol is not being "dethroned" by PDRN — it remains the best-studied anti-aging active in dermatology. But PDRN fills the gap for people who cannot tolerate retinol and offers a complementary mechanism for people who can. They are allies, not competitors.
PDRN vs Peptides: Broad Spectrum vs Surgical Precision
The peptide category is enormous — from signal peptides (Matrixyl, copper peptides) to neurotransmitter-inhibiting peptides (Argireline, SYN-AKE) to carrier peptides — each with a different mechanism. Comparing "PDRN" to "peptides" is like comparing one precision instrument to an entire toolbox [5].
Peptides That Overlap with PDRN's Territory
| Peptide Type | Mechanism | PDRN Comparison |
|---|---|---|
| Signal Peptides (Matrixyl 3000) | Fragment collagen/elastin sequences trick fibroblasts into producing more | PDRN achieves similar fibroblast activation but through A2A receptor, not decoy fragments |
| Copper Peptides (GHK-Cu) | Copper delivery for enzymatic collagen cross-linking + SOD activity | PDRN achieves collagen synthesis but not copper-dependent cross-linking; copper peptides achieve cross-linking but not A2A-mediated angiogenesis |
| Neuropeptides (Argireline) | Inhibit SNARE complex, reducing muscle contraction | PDRN has no muscle-relaxing effect — these are complementary, not overlapping |
The Stacking Logic
The most advanced regenerative formulations combine PDRN with targeted peptides — PDRN as the broad-spectrum regenerative foundation, peptides as the precision instruments layered on top:
- PDRN + Matrixyl 3000: A2A-mediated fibroblast activation + collagen-fragment signaling
- PDRN + Copper Peptides: Regeneration + enzymatic collagen maturation
- PDRN + Argireline: Tissue repair + expression line relaxation
This stacking approach is increasingly common in Korean aesthetic dermatology, where PDRN skin boosters are combined with peptide serums for comprehensive anti-aging protocols.
Verdict
PDRN and peptides are not competitors — they are natural formulation partners. PDRN provides the broad regenerative signal; peptides provide the targeted functional enhancements. In B2B formulation, the combination of PDRN + signal peptides is one of the most technically defensible anti-aging stacks available.
PDRN vs Azelaic Acid: Regeneration vs Clarification
Azelaic acid is a dicarboxylic acid with anti-inflammatory, antibacterial, and tyrosinase-inhibiting properties. It is commonly used for acne, rosacea, and hyperpigmentation — conditions where inflammation is a central driver [6].
Mechanism Comparison
| Dimension | PDRN | Azelaic Acid |
|---|---|---|
| Primary Mechanism | A2A receptor activation (regenerative) | Tyrosinase inhibition + antimicrobial |
| Anti-inflammatory | NF-κB suppression (broad) | ROS scavenging + kallikrein inhibition |
| Acne | Indirect (tissue repair) | Direct (antibacterial against C. acnes) |
| Hyperpigmentation | Indirect (improved skin quality) | Direct (tyrosinase inhibition) |
| Skin Texture | Collagen remodeling | Keratolytic (mild exfoliation) |
| Irritation Potential | None | Mild (tingling, dryness) |
These two ingredients have surprisingly complementary profiles: azelaic acid clears the problem (acne, pigmentation, rosacea flare-ups), while PDRN repairs the damage (post-inflammatory erythema, barrier repair, collagen restoration).
Verdict
They should be used together, not compared as alternatives. Azelaic acid in the AM (or alternating nights), PDRN in the PM.
PDRN vs PRP (Platelet-Rich Plasma): Defined vs Personalized
PRP is autologous — derived from the patient's own blood — and contains a personalized mixture of growth factors (PDGF, TGF-β, VEGF, EGF) concentrated from platelets. It has been used for decades in orthopedics, wound healing, and aesthetic medicine [7].
| Dimension | PDRN | PRP |
|---|---|---|
| Composition | Defined (DNA fragments, >95% purity) | Variable (patient-dependent growth factor profile) |
| Standardization | High (chemical specification) | Low (depends on patient age, health, collection protocol) |
| Source | Salmon milt (manufactured) | Patient blood (point-of-care) |
| Mechanism | A2A receptor activation | Multiple growth factor receptors |
| Shelf Life | Years (lyophilized powder) | Hours (fresh preparation) |
| Clinical Evidence | Strong (RCTs) | Strong for some indications, mixed for aesthetics |
| Cost | Moderate | Low (materials) + clinical time |
PRP has a conceptual elegance — using the body's own healing signals — but its variability is both its strength and its weakness. Two PRP preparations from the same patient on different days may have different growth factor concentrations. PDRN offers reproducibility that PRP cannot match, which is why manufacturers and formulators prefer it for commercial products.
Master Comparison Table
| Feature | PDRN | Exosomes | EGF | Retinol | Peptides | Azelaic Acid |
|---|---|---|---|---|---|---|
| Mechanism | A2A receptor | Cargo delivery | EGFR | RAR/RXR | Variable | Tyrosinase + antimicrobial |
| Clinical Evidence | ★★★★★ | ★★ | ★★★ | ★★★★★ | ★★★★ | ★★★★ |
| Safety Profile | ★★★★★ | ★★★ | ★★★ | ★★★ | ★★★★★ | ★★★★ |
| Standardization | ★★★★★ | ★★ | ★★★★ | ★★★★★ | ★★★★ | ★★★★★ |
| Irritation-Free | ★★★★★ | ★★★★ | ★★★★ | ★★ | ★★★★★ | ★★★ |
| Regulatory Clarity | ★★★★★ | ★★ | ★★★ | ★★★★★ | ★★★★★ | ★★★★★ |
| Cost-Effectiveness | ★★★★ | ★★ | ★★★ | ★★★★★ | ★★★★ | ★★★★★ |
| Vegan Option | L-PDRN | Yes (plant) | No (recombinant exists) | Yes | Yes (most) | Yes |
Formulating with PDRN: B2B Decision Framework
When building a product line around regenerative skincare, the decision is not "which one" — it is "what combination, in what format, for what consumer segment."
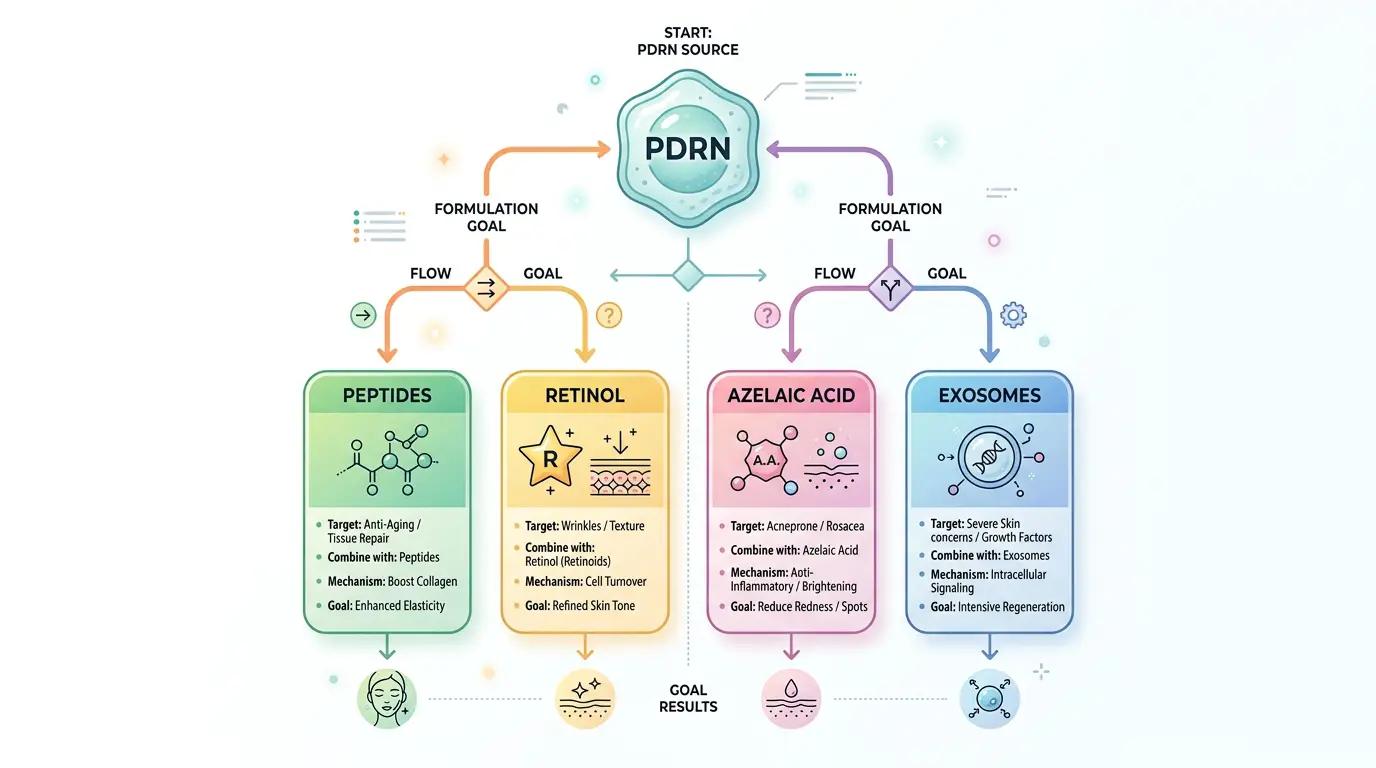
Decision Tree
- Need clinical evidence for claims? → PDRN (20+ years of data)
- Need irritation-free option for sensitive skin? → PDRN (zero irritation profile)
- Targeting vegan/clean beauty segment? → Consider L-PDRN or plant-derived peptides
- Building a premium injectable line? → PDRN or PDRN + exosome combination
- Adding anti-aging to an existing retinol line? → PDRN as complementary recovery-night product
- Need broad-spectrum regenerative foundation for a serum? → PDRN + signal peptides
The PDRN Product Development Advantage
For brands sourcing PDRN as a bulk raw material, the ingredient's characteristics translate to formulation and marketing advantages:
- Stability: Lyophilized PDRN is stable at room temperature for extended periods, reducing cold-chain logistics complexity
- Compatibility: Water-soluble, compatible with most cosmetic ingredients including HA, glycerin, niacinamide, panthenol, and peptides
- Claims support: 20+ years of published clinical literature provides a defensible evidentiary foundation for product claims
- Differentiation: In a market saturated with retinol and vitamin C products, PDRN offers genuine mechanistic novelty that consumers can understand ("salmon DNA skin repair")
Source pharmaceutical-grade PDRN powder from GINKVORA — full COA, TDS, and regulatory documentation available for your product development.
Related Articles
- What Is PDRN? The Complete Guide to Salmon DNA in Skincare — Deep dive into PDRN's mechanism, clinical evidence, and skincare applications
- Glabridin Before and After: 16× Stronger Than Kojic Acid — Head-to-head potency comparison for another high-performance cosmetic active
- Why Your Whitening Serum Underperforms: The 5-Pathway Strategy — Multi-mechanism formulation approach using complementary actives
References
Squadrito F, Bitto A, Irrera N, et al. Pharmacological Activity and Clinical Use of PDRN. Frontiers in Pharmacology. 2017;8:224. https://doi.org/10.3389/fphar.2017.00224
Théry C, Witwer KW, Aikawa E, et al. Minimal Information for Studies of Extracellular Vesicles 2018 (MISEV2018). Journal of Extracellular Vesicles. 2018;7(1):1535750. https://doi.org/10.1080/20013078.2018.1535750
Cohen S. The Epidermal Growth Factor (EGF). Cancer. 1983;51(10):1787-1791. https://doi.org/10.1002/1097-0142(19830515)51:10<1787::AID-CNCR2820511004>3.0.CO;2-A
Mukherjee S, Date A, Patravale V, et al. Retinoids in the Treatment of Skin Aging: An Overview of Clinical Efficacy and Safety. Clinical Interventions in Aging. 2006;1(4):327-348. https://doi.org/10.2147/ciia.2006.1.4.327
Kim TH, Kim JY, Bae JH, et al. Biostimulatory Effects of Polydeoxyribonucleotide for Facial Skin Rejuvenation. Journal of Cosmetic Dermatology. 2019;18(6):1767-1773. https://doi.org/10.1111/jocd.12958
Fitton A, Goa KL. Azelaic Acid: A Review of Its Pharmacological Properties and Therapeutic Efficacy in Acne and Hyperpigmentary Skin Disorders. Drugs. 1991;41(5):780-798. https://doi.org/10.2165/00003495-199141050-00007
For a comprehensive overview of PDRN's mechanism and clinical evidence, see What Is PDRN? The Complete Guide to Salmon DNA in Skincare.